Clinical diagnostics teams rarely struggle because they lack software. More often, they struggle because the work is split across too many systems. Sample records live in one place, instrument outputs in another, SOPs somewhere else, and key steps still depend on spreadsheets, email, paper logs, or manual review.
That split shows up fast in day-to-day lab work. A team cannot trace a sample cleanly from intake to result. A PCR file still has to be copied by hand into a report. A lab preparing for accreditation has the work done, but not the evidence linked in a way an auditor can review without friction. A workflow exists on paper, but the software does not match what actually happens at the bench.
Across multiple Scispot diagnostics customers, five problems came up again and again. They appeared in different forms, but the pattern was consistent. Clinical teams needed one connected operating system for sample lineage, workflow execution, instrument data, reporting, and compliance evidence, not a patchwork of tools that each solved one narrow step.
1. Fragmented sample tracking and chain of custody
The first problem was traceability. As labs moved beyond simple intake and storage, they had to keep clear links between patients, orders, source samples, aliquots, child samples, controls, locations, tests, and final results. That sounds basic until samples branch into multiple assays, move across locations, or generate derivative materials that also need to stay tied back to the original record.
In practice, we saw labs struggling to keep IDs aligned across accessioning, extraction, plate setup, and reporting. Teams wanted stronger continuity between sample IDs, well IDs, controls, extracted derivatives, and final reports. Others needed end-to-end traceability from collection sites through shipping and processing. Some needed block-to-slide lineage across parallel histology and molecular workflows.
When that chain of custody lives in memory, spreadsheets, or disconnected systems, labs lose time and increase risk. Staff have to reconstruct lineage by hand. Reviews take longer. Auditors and clinical teams have to ask basic questions that should already be answerable in the system.
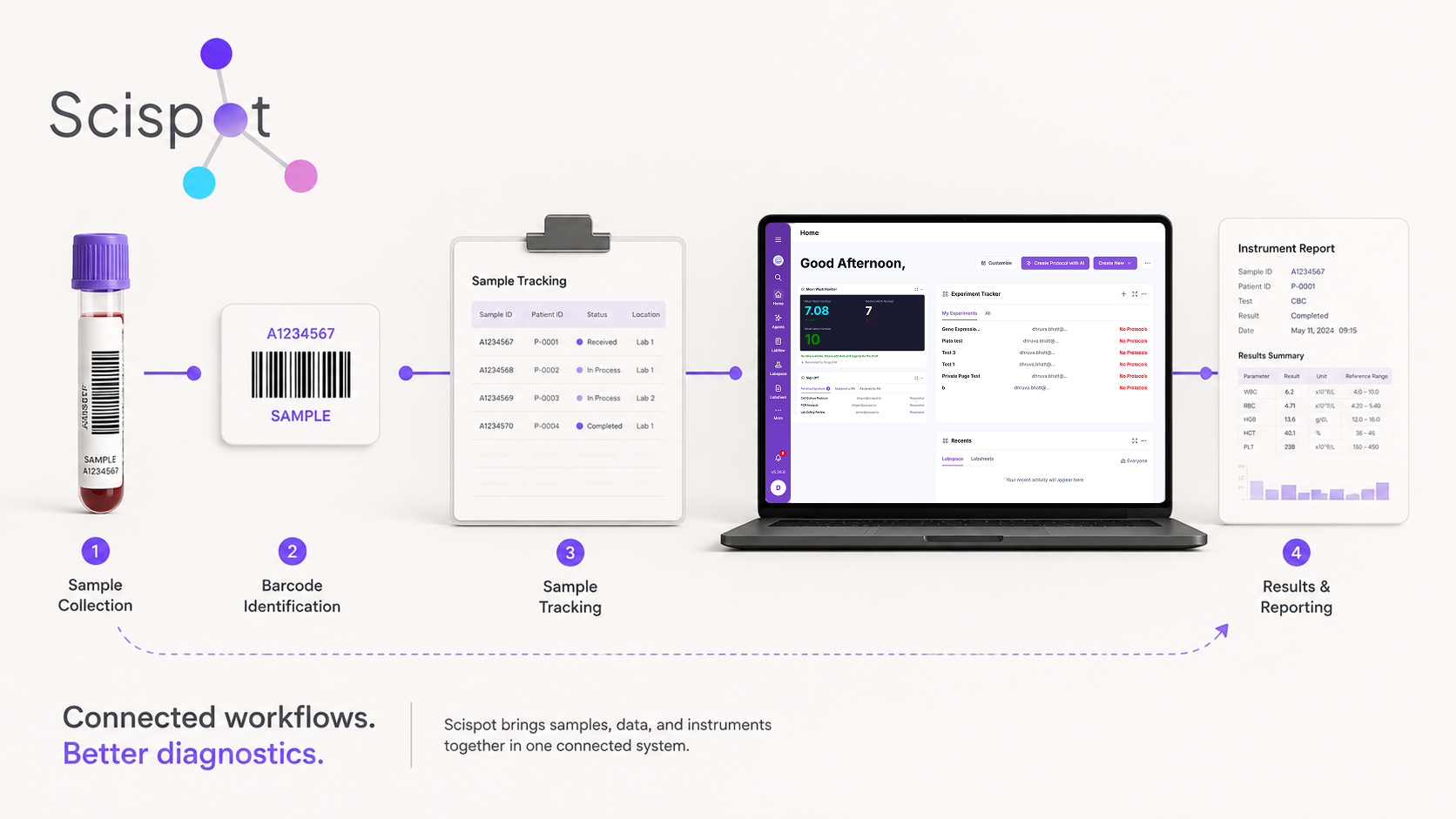
Scispot addresses this with sample managers, parent-child logic, Labflows or Lab Spaces, barcode workflows, manifest structures, and location tracking that match actual lab movement. Implementations typically focus on accessioning, order and sample management, child sample creation, branching into tests, and storage hierarchies that reflect the real freezer and storage layout.
Diagnostics labs do not just need to store records. They need to preserve relationships between records. Once a lab has parent and child samples, controls, batch handling, assay branching, and distributed processing, weak lineage becomes a daily operational problem, not just a data-model issue.
2. Manual, error-prone intake and data ingestion
The second problem was intake. Many teams were still dealing with manual submissions, hospital spreadsheets, email attachments, external forms, or legacy workflows that forced staff to re-enter the same information multiple times before the lab could even start work.
We saw labs that lacked pre-accessioning portals, which meant sample submission data had to be transcribed manually before downstream work could begin. Others were ingesting multi-sheet Excel files from external partners and trying to link patient, specimen, order, and result data into a usable structure. Some sites sent data in inconsistent formats across email, attachments, and older systems, which made “simple” intake work far harder than it needed to be.
Manual intake creates more than delay. It creates duplication, formatting errors, missed fields, and extra review steps. Labs pay for it twice: once during data entry, and again when the bench team has to stop and resolve what should have been structured correctly at the start.
Scispot addresses this with forms, imports, field mapping, API-based ingestion, scripts, status automations, and data models built around patients, specimens, orders, and results. In practice, that means well-designed submission forms tied to canonical internal IDs, manifest imports that map columns correctly, and ingestion flows that preserve traceability instead of scattering data across ad hoc sheets.
Labs often assume the main bottleneck starts once a sample reaches extraction or assay setup. In reality, intake design shapes everything downstream. If IDs are inconsistent at submission, if records arrive in the wrong format, or if order and specimen data are not linked cleanly at the start, the rest of the workflow becomes harder than it needs to be.
3. Instrument integration and result harmonization
The third problem was the gap between instruments and operations. Many labs could generate instrument data, but they still lacked a repeatable way to bring that data into a workflow where it could support QC, review, reporting, and release.
A common pattern we saw: after PCR or qPCR runs, analysts had to read instrument results and enter them manually, pushing turnaround times out and creating extra review burden. In multiplex or multi-instrument setups, teams had to reconcile different output formats into one view before they could decide whether runs passed QC. In more advanced environments, labs needed reliable qPCR integration with correct file handling, replicate averaging, QC checks, run IDs, and structured writing of results back into sample records.
This is where many lab software projects fall short. Reading a file is not enough. Instrument data has to land in the right record, map to the right sample or accession, trigger the right QC logic, and support reporting without forcing analysts into another round of spreadsheet work.
Scispot addresses this through file-based ingestion design, smart actions, QC rules, parser logic, and integration support across PCR, qPCR, and other instruments. That can include mapping well layouts to plate manifests, applying pass/fail logic based on thresholds, handling controls correctly, and pushing structured data back into the sample manager where it belongs.
Once instrument outputs are structured and traceable inside the workflow, labs can reduce transcription errors, tighten QC, and make review and reporting less brittle. The issue is not only integration. It is harmonization inside the lab’s actual operating model.
4. Audit readiness, compliance, and documentation burden
The fourth problem was compliance overhead. Many customers were operating in, or preparing for, regulated environments that required more than good science. They needed proof. That meant versioned SOPs, audit trails, permissions, training records, controlled documentation, sign-offs, and evidence that workflows were complete and governed.
We saw labs under pressure from accreditation timelines, internal mock audits, and policy requirements. In those contexts, teams needed work instructions, protocol templates, training certificates, documentation, and user-facing manuals to be audit-ready. They also needed IQ/OQ/PQ records, trust-vault style evidence, and sign-off behavior that reflected how work actually progressed.
Separate systems make this harder. If SOPs live in shared drives, training evidence lives in another folder, workflow data lives in the LIMS, and sign-off records are managed elsewhere, labs end up rebuilding the same narrative every time someone asks for proof. The work may exist, but the evidence is scattered.
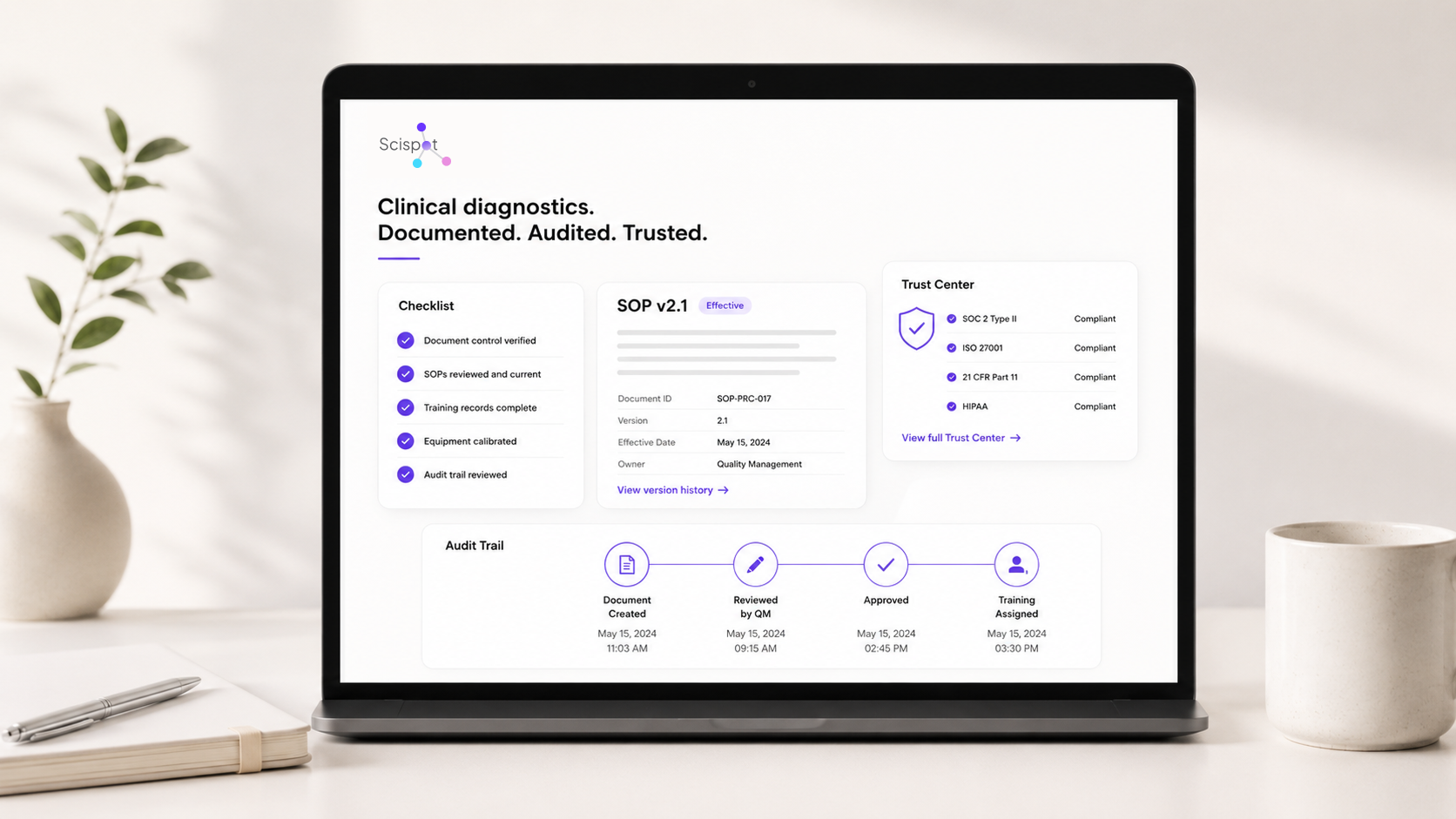
Scispot addresses this with trust centers, QMS-oriented documentation, audit logs, training artifacts, permissions models, controlled protocols, sign-offs, template locking, versioning, and workflow-linked evidence. Labs use the platform to keep work and proof together: protocols are versioned and controlled, training and IQ/OQ records sit beside the workflows they support, and audit logs show how data and status changed over time.
For diagnostics labs, audit readiness is not a separate project from operations. It is the operational system viewed under scrutiny. Labs move faster when the same system that runs the work also keeps the evidence attached to that work.
5. Workflow rigidity and automation debt
The fifth problem was software that did not match how labs actually work. Even when a platform had the right high-level modules, teams still ran into friction if views were awkward, filters were too rigid, automations were brittle, labels were cumbersome, or workflows forced the bench to adapt to the tool instead of the other way around.
We saw teams hitting limits with filtering logic, column management, shared workstation behavior, and automation triggers that broke whenever schemas changed. Some labs had accumulated dozens of overlapping automations and scripts that created duplicate rows, silent failures, and hard-to-debug behavior. Others found that basic day-to-day tasks—like assigning locations, printing labels, or stepping through protocols—felt harder in software than they did on paper.
This is easy to dismiss as UX cleanup, but it is not minor. In a clinical or high-throughput environment, small workflow mismatches create workarounds. Workarounds create duplicate steps, duplicate records, manual checks, and hidden quality risk.
Scispot addresses this through tailored configuration, protocol templates, barcode and label printing, workflow redesign, view restructuring, automation audits, and responsive implementation support. That often means reviewing how staff actually work, adjusting flows and views to match that reality, consolidating automations, and removing brittle logic so everyday tasks become simpler and safer.
Diagnostics teams do not just need features on a checklist. They need software that reflects how samples move, how staff review work, how instruments feed results, and how exceptions are handled on real days in the lab.
What these five problems have in common
These are not isolated software complaints. They are connected operating problems. Weak intake affects traceability. Poor instrument integration creates reporting and QC burden. Split documentation makes audit readiness harder. Rigid workflows push teams back into spreadsheets and manual review.
The strongest pattern across these stories is not one missing module. It is the need for a connected operational system. Labs are trying to tie sample movement, instrument output, reporting, documentation, inventory, and audit evidence together in one place, with enough flexibility to match real lab work.
Scispot’s role across these customers is to help build that connected layer. In some cases, the value shows up in clearer sample lineage. In others, it shows up in intake structure, parser design, QC logic, audit preparation, or workflow redesign. The exact implementation varies by lab, but the recurring need is the same: fewer handoffs, fewer disconnected records, and a more usable system of record for diagnostics operations.
For clinical diagnostics teams, that is the real shift. The goal is not to add another tool. The goal is to reduce the number of places where critical lab work can fall apart.


.webp)